
Background
- Tears of the latissimus dorsi (LD) and teres major (TM) muscles occur in high level throwers.
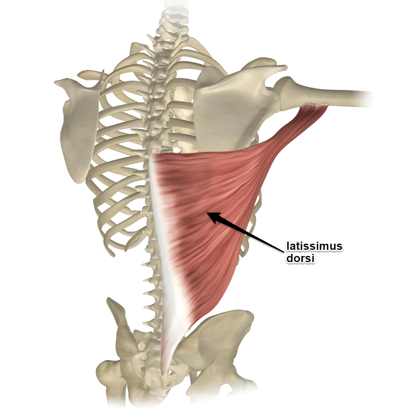
- The LD originates from the lower thoracic spine, lower ribs, and iliac crest.
- The LD inserts on the inner part the humerus bone just below the glenohumeral joint.
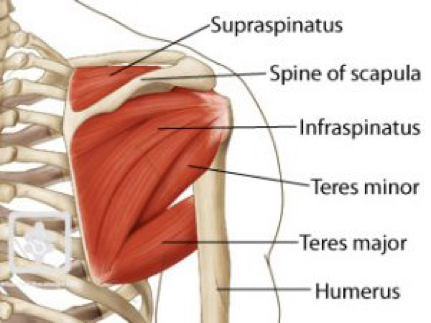
- The TM originates bottom of the scapula and inserts on the inside part of the humerus adjacent to LD.
- The LD/TM tendon anatomic relationship is variable.
- The LD/TM tendons are often adherent to one another.
- On occasion TM tendon can actually insert into the LD tendon.
Function
- The primary function of the LD/TM is humeral extension, adduction, and internal rotation.
- Both the LD and TM muscles are strong internal rotators of the humerus. These muscles are critically important to generating the tremendous humeral rotation that creates throwing velocity.
- The muscles are most active during the late cocking and acceleration phases of the pitching cycle.
- LD and TM injuries can also occur in other sporting activities including water skiing, wakeboarding, tennis, and rock climbing.
CLINICAL EVALUATION
History
- The athlete may experience a pop or the acute onset of pain in the back or their shoulder.
- Sometimes the athlete may experience fatigue in the shoulder/back region with loss of velocity and control.
Physical Examination
- Bruising and swelling may be noted overlying the latissimus.
- Asymmetry of the posterior axillary fold may be observed.
- Occasionally, the TM will demonstrate medial retraction.
- The entire course of the LD and TM should then be palpated for tenderness.
- Weakness is elicited in shoulder adduction and extension and, to a lesser degree, in internal rotation.
- Pain is often reproduced with resisted shoulder extension and adduction.
Video 2. Normal exam of Latissimus Dorsi and Teres Major.
Video 3. Patient with Teres Major rupture with abnormal contour.
Video 4. Patient with Lattisimus Dorsi Tear.
Imaging
- MRI can evaluate the LD/TM over the entire course of the muscle-tendon unit.
- We recommend a shoulder MRI that extends to the lateral chest wall and if necessary a chest MRI to follow the entire latissimus tendon and muscle.
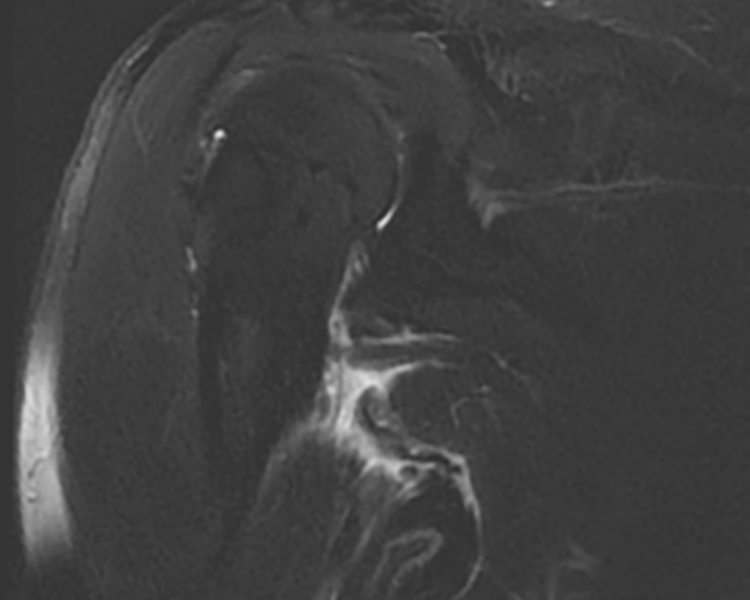
- MRI can demonstrate tendon tearing or muscle strain or a combination of both.
Below figure shows a muscle strain
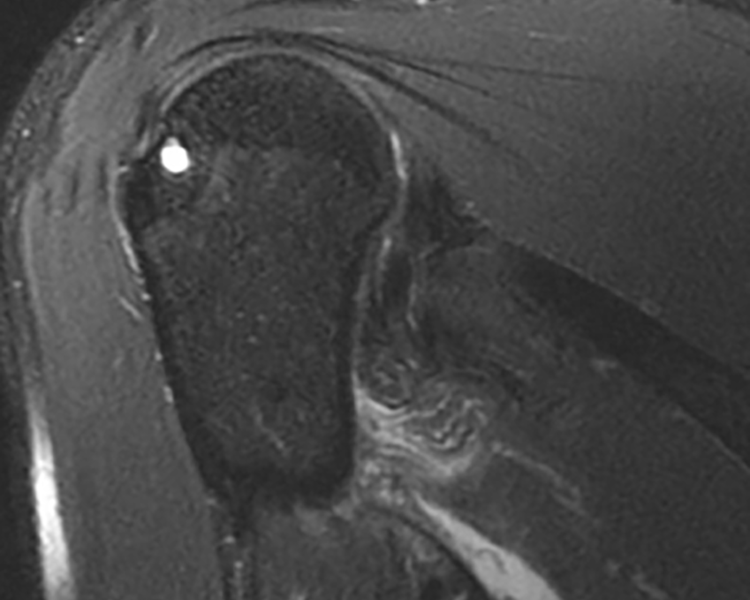
Below figure shows a tendon tear.
Video 5. MRI shows Latissimus Dorsi Tendon tear.
Treatment
If you are experiencing intense shoulder pain or feelings of instability, you may require treatment to repair and prevent any damage. You should cease all strenuous activity and make an appointment with your doctor immediately. Treatment may include immobilization,medication,rehabilitation, or surgery.
Nonoperative
- Strains are treated with rest, cryotherapy, anti-inflammatory medications, modalities, and shutdown from throwing.
- When pain is resolved, ROM is restored with therapy and core muscle and lower body strengthening is initiated.
- Isometric exercises for the LD/TM are initially performed and progressed to resistance exercises.
- Once full motion and strength are regained, a progressive throwing program is initiated.
- The length of time for each phase varies by player.
- The time frame for return to competition after the successful nonoperative treatment of an LD/TM injury depends on the severity of injury and can be 3 months or longer.
- We have used PRP to accelerate healing for LD muscle strains
Surgical Indications
- Surgical repair of the LD/TM tendon avulsion tears can be offered to high level athletes.
- Failure of non-operative treatment or significant tendon retraction are indications for surgery.
Surgical Technique
- The tendon is retrieved and anatomically repaired to its normal insertion site on the humerus bone.